'NOT SUFFICIENT' Alison Smart / iStock HEALTH Utah mom fights for her daughter’s access to discontinued diabetes medication: ‘Life-saving'
DREAM DIET iStock HEALTH Having trouble sleeping? It could be for this surprising reason, experts say
JUICY DISCOVERY iStock HEALTH Drinking 100% orange juice is linked to surprising health benefits, study finds
WATER HAZARD iStock HEALTH 'Forever chemicals' found in US drinking water, map shows 'hot spots' of highest levels
HEALTH 1 hour ago CDC warns of extreme heat dangers amid ‘record-breaking high temperatures’ Many regions across the U.S. experienced “record-breaking high temperatures" in 2023 due to extreme heat, according to the CDC. Experts share risk factors and safety tips.
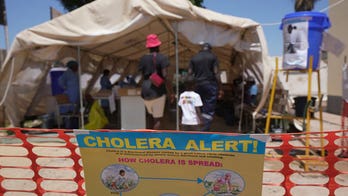
World Health Organization 8 hours ago World Health Organization approves updated cholera vaccine to combat surge in cases The World Health Organization has approved a new version of a cholera vaccine that could help address a surge in cases that has depleted the global vaccine stockpile.
HEALTH 10 hours ago Utah mom fights for her daughter’s access to discontinued diabetes medication: ‘Life-saving' A Utah mother is fighting for her teen daughter’s access to diabetes medicine after it was discontinued. Alison Smart, plus other parents and medical experts, discussed the risks and options.
VIDEO 1 day ago Milk carton art campaign spotlights tech risks for youth Artist David Cicirelli and ‘The Anxious Generation’ author Jonathan Haidt join ‘America’s Newsroom’ to discuss the risks social media poses to children’s mental health.
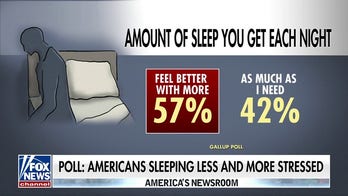
VIDEO 1 day ago Why Dr. Siegel treats stress and sleeplessness as one issue Fox News contributor Dr. Marc Siegel breaks down the ‘cycle of worry’ as a poll finds Americans are sleeping less and stressing more.
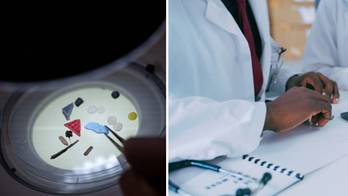
World Health Organization 1 day ago World Health Organization, experts reach landmark agreement on how to define airborne diseases The World Health Organization and around 500 experts have established a consensus on what it means for a disease to spread through the air, officials said.
HEALTH 1 day ago Having trouble sleeping? It could be for this surprising reason, experts say What you eat can have an impact on your sleep. Two sleep experts shared foods that promote sleep, foods to avoid, and how to know if your dietary choices are keeping you up at night.
HEALTH 1 day ago Study finds evidence of microplastics in brains and other organs Two recently-published studies investigated how microplastics can find their way inside the organs of both humans and mice, and what the potential impact can be.
10 hours ago Utah mom fights for her daughter’s access to discontinued diabetes medication: ‘Life-saving'
1 day ago World Health Organization, experts reach landmark agreement on how to define airborne diseases
3 days ago Ozempic babies: Women claim weight-loss drugs are making them more fertile and experts agree
April 11 Puberty blockers could cause long-term fertility and health issues for boys, study finds: 'May be permanent'
April 9 Cancer rates rising in young people due to ‘accelerated aging,’ new study finds: ‘Highly troubling’
April 7 Dutch woman, 28, to be euthanized over mental illness after psychiatrist said it will 'never' get any better
April 6 Vaccinating migrants like US children would have prevented disease outbreaks at Chicago shelters: experts
April 5 CDC issues bird flu health alert to clinicians, state health departments, public after Texas farmer infected
April 4 Massachusetts man, recipient of first successful pig kidney transplant, is discharged from hospital
April 4 Cancer cases in the spotlight as White House declares April 2024 'Cancer Prevention and Early Detection Month'
April 3 Bird flu pandemic in future? EU warns of potential spread to humans due to 'lack of immune defense’
April 3 Baby sleep dangers revealed in new study as nearly 70% of infant deaths were due to co-sleeping
April 2 Federal government says hospitals must obtain written consent for exams on pelvis, other sensitive areas
April 1 CDC warns of invasive bacterial outbreak amid spike in cases and fatality rates: 'Rare but severe'
April 1 Pneumonia misdiagnoses are common among hospitalized adults, study finds: There are 'implications'
March 31 Health's weekend read includes Taylor Swift's impact amid brain surgery, seniors’ health struggles and more
March 30 New Jersey woman sings Taylor Swift hits while awake during brain surgery: 'Eras Tour' in the O.R.
March 29 Top UK health official urges against eating whole Easter egg in 'one go' hit with backlash: 'Life too short'
March 28 Health care is ‘overwhelmingly complex’ for older adults, experts say: ‘Ever-increasing hurdle’
March 26 Cold therapy techniques come under hot scrutiny by researchers: 'Overall benefits remain uncertain'
March 25 FDA proposes ban on electrical shock devices used to stop aggressive behavior for the second time
March 25 New blood test shows high accuracy for colorectal cancer detection, study finds: ‘Not interchangeable’
March 25 Daily marijuana smokers face higher risk of heart attack, stroke, says American Heart Association study
March 22 Princess Kate Middleton undergoing ‘preventative chemotherapy’ after cancer diagnosis: ‘Stronger every day’
March 16 Potentially fatal dog parasite found in part of Colorado River for first time, having spread from other states
March 14 Man suffering from migraines found to have tapeworms in brain after consuming partially cooked bacon: study
March 13 Tommy John surgery continues to save baseball careers 50 years after its debut: 'Revolutionary'